¶ NAD+ Precursors: The Strategic Guide
¶ At a Glance
What are they? Molecules that your body converts into NAD+, the critical "fuel" for cellular energy and longevity enzymes (Sirtuins). NAD+ levels drop by ~50% as you age, driving mitochondrial dysfunction.
The Goal: Restore youthful NAD+ levels to support energy, DNA repair, and metabolic resilience.
The Challenge: NAD+ itself is not well-absorbed orally. You must take a precursor that can cross cell membranes and be converted inside the cell.
¶ Executive Dashboard: Choosing Your Strategy

Not all NAD+ boosters are equal. The choice depends on your budget, tolerance for side effects, and specific health goals.
¶ The "Traffic Light" Comparison
| Intervention | Cost | Bioavailability | Side Effects | Best For | Verdict |
|---|---|---|---|---|---|
| NMN (Nicotinamide Mononucleotide) |
$$$ | High (Direct precursor) |
Minimal | All-Around Longevity Those wanting the most direct oral route. |
🟢 Go The current gold standard for direct efficacy. |
| NR (Nicotinamide Riboside) |
$$$ | High (Efficient conversion) |
Minimal | Established Data Those who prefer the most human safety data. |
🟢 Go Excellent, clinically validated alternative to NMN. |
| Niacin (Nicotinic Acid) |
$ | Variable (Different pathway) |
Flushing (Skin redness/heat) |
Budget / Lipids Those needing cholesterol support + NAD+ on a budget. |
🟡 Caution Uncomfortable flush limits the high doses needed for NAD+. |
| NAD+ IV Therapy (Intravenous Drip) |
$$$$ | 100% (Blood) (Uncertain cellular uptake) |
Nausea, Anxiety (during infusion) |
Acute Recovery Detox, withdrawal, or elite athlete recovery. |
🔴 Stop/Think Expensive and invasive. Does it actually enter cells? |
¶ Quick Protocols
- The "Gold Standard" Protocol:
- AM: 500mg–1g of NMN or NR (enteric coated or liposomal preferred).
- Cofactors: TMG (Trimethylglycine) 500mg to support methylation.
- The "Budget" Protocol:
- AM/PM: 50-100mg Niacin (Nicotinic Acid) with food. Warning: Will cause flushing.
¶ The Debate: NR vs. NMN vs. IV
¶ 1. The NMN vs. NR Rivalry
The scientific community is divided between these two giants.
- The Argument for NMN: It is one step closer to NAD+ than NR. Some research suggests a specific transporter (Slc12a8) allows NMN to enter cells directly, bypassing the conversion step required for NR.[1]
- The Argument for NR: It has more published human clinical trials confirming safety and bioavailability. Skeptics argue NMN must be broken down into NR before entering the cell anyway, making NR the "true" precursor.[2]
- The Reality: Both effectively raise NAD+ levels in human blood.[3][4] The choice often comes down to personal response and cost.
¶ 2. The "Niacin Flush" Dilemma
Niacin (Vitamin B3) is dirt cheap and raises NAD+ via the Preiss-Handler pathway, bypassing the enzyme (NAMPT) that often fails in aging.
- Why isn't it #1? To get longevity-level NAD+ boosts, you often need high doses (500mg+). This causes an intense "flush" (burning, red skin) mediated by the GPR109A receptor. While harmless, it is intolerable for many daily users.
- The Lipid Bonus: Unlike NR/NMN, Niacin significantly lowers LDL cholesterol and triglycerides, offering a dual benefit for cardiovascular health.
¶ 3. The IV Controversy
NAD+ Clinics offer infusions costing $500+.
- The Claim: "100% absorption" bypasses the gut.
- The Science Gap: NAD+ is a massive molecule. It lacks a transporter to get into cells (except maybe in neurons/heart). It likely gets broken down into NMN/NR in the blood, then re-synthesized inside cells.
- Verdict: You might be paying a premium for an expensive way to generate NMN in your bloodstream.
¶ Deep Dive: Mechanisms & Science
¶ The Pathways to NAD+
Your body makes NAD+ through three distinct roads. Aging blocks the main road, forcing us to use detours.
-
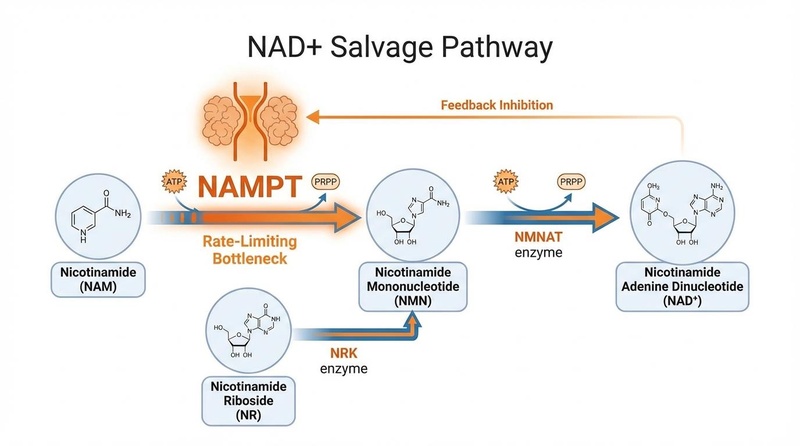
The Salvage Pathway (NMN & NR):
- Mechanism: Recycles "used" NAD+ (Nicotinamide) back into fresh NAD+.
- Bottleneck: The enzyme NAMPT slows down with age and inflammation. NMN and NR enter this pathway after the bottleneck, restoring flow.
- Key Insight: This is why "just taking Vitamin B3 (Nicotinamide)" doesn't work well for longevity—it gets stuck at the NAMPT bottleneck.[5]
-
The Preiss-Handler Pathway (Niacin):
- Mechanism: Converts dietary Niacin into NAD+ via a different set of enzymes (NAPRT).
- Advantage: Completely independent of NAMPT. If your salvage pathway is blocked by inflammation, Niacin might actually work better than NMN/NR in specific tissues.[6]
-
The De Novo Pathway (Tryptophan):
- Mechanism: Converts amino acids into NAD+.
- Efficiency: Terrible. You need ~60mg of Tryptophan to make 1mg of NAD+. Not a viable longevity strategy.[7]
¶ Human Evidence Summary
| Outcome | Effect | Evidence Grade | Key Findings |
|---|---|---|---|
| Blood NAD+ Levels | ↑ Large | GRADE A | NR and NMN consistently double or triple blood NAD+ in humans within weeks.[3:1][4:1] |
| Insulin Sensitivity | ↑ Small | GRADE B | NMN improved muscle insulin sensitivity in prediabetic women (PMID: 33888596).[8] |
| Exercise Capacity | ↑ Mixed | GRADE C | Some improvement in VO2 max for amateur runners; other studies show no benefit.[9] |
| Inflammation | ↓ Small | GRADE C | NR showed reduction in inflammatory cytokines in some small trials.[10] |
| Longevity (Humans) | ? Unknown | Insufficient | No multi-year mortality trials exist yet. Evidence is extrapolated from biomarkers and animal data. |
¶ Safety & Methylation
- Methylation Depletion: Converting high doses of precursors requires methyl groups. Theoretically, this could deplete your body's methyl pool (raising Homocysteine).
- Solution: Many experts recommend taking TMG (Trimethylglycine) or Methyl-Folate with NMN/NR as an "insurance policy."
- Tumor Growth: NAD+ fuels all cells, including cancer cells. While NAD+ precursors do not cause cancer, there is a theoretical risk they could accelerate the growth of an existing active tumor. Avoid if undergoing active cancer treatment unless approved by an oncologist.
¶ References
Grozio, A., et al. (2019). Slc12a8 is a nicotinamide mononucleotide transporter. Nature Metabolism, 1(1), 47–57. https://www.nature.com/articles/s42255-018-0009-4 ↩︎
Trammell, S. A., et al. (2016). Nicotinamide riboside is uniquely and orally bioavailable in mice and humans. Nature Communications, 7, 12948. https://www.nature.com/articles/ncomms12948 ↩︎
Martens, C. R., et al. (2018). Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults. Nature Communications, 9(1), 1286. https://www.nature.com/articles/s41467-018-03421-7 ↩︎ ↩︎
Irie, J., et al. (2020). Effect of oral administration of nicotinamide mononucleotide on clinical parameters and nicotinamide metabolite levels in healthy Japanese men. Endocrine Journal, 67(2), 153-160. https://pubmed.ncbi.nlm.nih.gov/31685720/ ↩︎ ↩︎
Yoshino, J., et al. (2011). Nicotinamide mononucleotide, a key NAD+ intermediate, treats the pathophysiology of diet- and age-induced diabetes in mice. Cell Metabolism, 14(4), 528-536. https://pubmed.ncbi.nlm.nih.gov/21982712/ ↩︎
Bogan, K. L., & Brenner, C. (2008). Nicotinic acid, nicotinamide, and nicotinamide riboside: a molecular evaluation of NAD+ precursor vitamins in human nutrition. Annual Review of Nutrition, 28, 115-130. https://pubmed.ncbi.nlm.nih.gov/18429699/ ↩︎
Badawy, A. A. (2017). Kynurenine Pathway of Tryptophan Metabolism: Regulatory and Functional Aspects. International Journal of Tryptophan Research, 10. https://pubmed.ncbi.nlm.nih.gov/28469468/ ↩︎
Yoshino, M., et al. (2021). Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women. Science, 372(6547), 1224-1229. https://www.science.org/doi/10.1126/science.abe9985 ↩︎
Liao, B., et al. (2021). Nicotinamide mononucleotide supplementation enhances aerobic capacity in amateur runners: a randomized, double-blind study. Journal of the International Society of Sports Nutrition, 18(1), 54. https://jissn.biomedcentral.com/articles/10.1186/s12970-021-00442-4 ↩︎
Elhassan, Y. S., et al. (2019). Nicotinamide riboside augments the aged human skeletal muscle NAD+ metabolome and induces transcriptomic and anti-inflammatory signatures. Cell Reports, 28(7), 1717-1728. https://pubmed.ncbi.nlm.nih.gov/31412242/ ↩︎
Comments
Discussion