¶ Glucosamine
What is it? Glucosamine is a naturally occurring amino sugar and a fundamental building block of joint cartilage. It is widely supplemented to reduce joint pain, delay osteoarthritis progression, and, according to recent large-scale studies, potentially support cardiovascular health and longevity.
Will it help me? If you have mild-to-moderate knee osteoarthritis, the specific prescription crystalline glucosamine sulfate formulation may significantly reduce pain and improve function. Standard over-the-counter glucosamine hydrochloride is largely considered ineffective for joint pain. Habitual use may also offer systemic anti-inflammatory benefits, though more clinical trials are needed to confirm longevity effects.
¶ Safety & Contraindications 🛑
- Severe Drug Interaction: Glucosamine strongly interacts with Warfarin (Coumadin). It can potentiate the anticoagulant effect, leading to elevated INR values and an increased risk of severe bleeding. Patients on warfarin should generally avoid glucosamine or require strict INR monitoring.
- Shellfish Allergies: Most commercial glucosamine is derived from the exoskeletons of shellfish. While the allergen is usually in the meat, those with severe shellfish allergies should seek vegan/fungal-derived glucosamine alternatives.
- Diabetes Monitoring: Human trials show no significant negative effect on fasting blood glucose for most people, but individuals with diabetes should monitor their blood sugar levels closely when initiating supplementation.
¶ Protocol Card
- Standard Dosage: 1,500 mg per day.
- Preferred Form: Crystalline Glucosamine Sulfate (pCGS). The hydrochloride (HCl) form lacks the sulfate group necessary for specific cartilage benefits and fails to outperform placebo in meta-analyses.
- Administration: Typically taken as a single 1,500 mg dose once daily (to achieve peak plasma concentrations) or divided into three 500 mg doses.
- Cycling & Duration: Benefits for joint pain typically require 4–12 weeks of continuous use to become apparent. Clinical guidelines suggest reviewing treatment efficacy after 3 months; if no benefit is observed, discontinuation is recommended.
- Combination: Frequently paired with Chondroitin Sulfate, though recent network meta-analyses suggest combinations with Omega-3s or short-term NSAIDs may be more effective for acute pain management.
¶ Bottom Line
Glucosamine is a highly debated supplement where the formulation is everything. While generic glucosamine hydrochloride is generally ineffective for joint pain, high-quality crystalline glucosamine sulfate is recognized by European guidelines as a valid first-line background therapy for knee osteoarthritis. Emerging data also links habitual glucosamine use to reduced risks of cardiovascular mortality, likely due to its systemic anti-inflammatory and autophagy-inducing properties.
¶ The "Why": Benefits & Outcomes
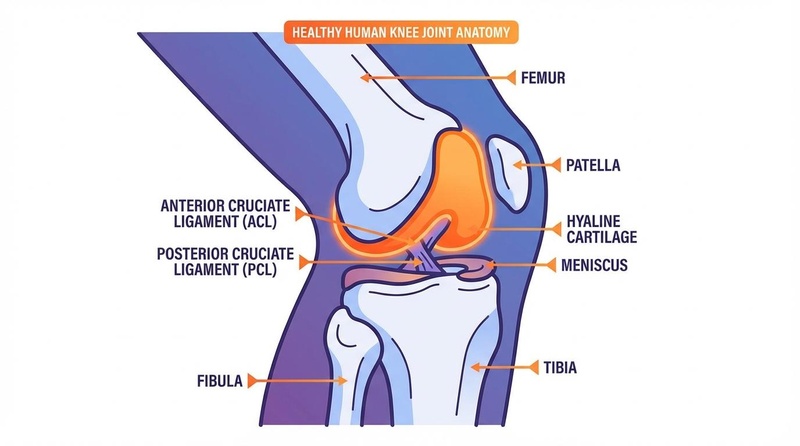
¶ 1. Osteoarthritis and Joint Pain
The most established use of glucosamine is in the management of osteoarthritis (OA), particularly of the knee. Glucosamine acts as a substrate for the biosynthesis of glycosaminoglycans (GAGs) and proteoglycans, essential structural components of articular cartilage and synovial fluid [1]. When the correct formulation is used, it has been shown to reduce joint pain, improve mobility, and potentially delay the structural progression of joint space narrowing over several years [2][3].
¶ 2. Cardiovascular Health and Longevity
Recent large-scale epidemiological studies have unveiled unexpected systemic benefits. A landmark prospective study using UK Biobank data (over 466,000 participants) found that habitual glucosamine use was associated with a 15% lower risk of total cardiovascular disease (CVD) events and a 22% reduction in CVD-related death [4]. Similar findings from the US NHANES data showed a 39% reduction in all-cause mortality associated with regular use (for over a year) [5]. While these studies are observational, the magnitude of mortality reduction is notable and currently under investigation for causal mechanisms.
¶ Reality Check: The Formulation Divide
The clinical utility of glucosamine is characterized by a stark "Atlantic Divide" in medical opinion, almost entirely stemming from the specific chemical formulation used in trials:
- Crystalline Glucosamine Sulfate (pCGS): This specific formulation, often stabilized with sodium chloride (the "Rotta preparation"), is approved as a prescription drug in Europe. It demonstrates high bioavailability and consistent clinical efficacy for reducing OA pain [6][7]. The European Society for Clinical and Economic Aspects of Osteoporosis (ESCEO) strongly recommends pCGS as a Step 1 background therapy for knee OA [8].
- Glucosamine Hydrochloride (HCl): This is the most common, cheaper over-the-counter form in the United States. Multiple meta-analyses, including Cochrane reviews, confirm that glucosamine HCl fails to show benefits superior to placebo for osteoarthritic pain [9][10]. Consequently, American guidelines (ACR, OARSI) generally recommend against glucosamine use, as they often do not differentiate between the commercial HCl supplements and the prescription sulfate form [11][12].
The takeaway: If you are taking glucosamine for joint health, verify that the label specifies "Glucosamine Sulfate" and ideally look for a stabilized crystalline form.
¶ Practical Integration
- Food Sources: You cannot get therapeutic amounts of glucosamine from food. It is derived from the shells of crabs, oysters, and shrimp, which are not typically consumed.
- Timing: Can be taken with or without food. Taking it with meals may reduce the risk of mild gastrointestinal upset.
- Patience is Key: Glucosamine is not an acute analgesic (like ibuprofen). It operates by modulating biological pathways and requires a minimum of 4 to 8 weeks of consistent daily use to assess any meaningful reduction in joint pain [13].
Vegetarian and Vegan Options
Because standard glucosamine is sourced from shellfish, it is inherently non-vegan. However, commercial processes now exist to synthesize glucosamine from the fungus *Aspergillus niger* or through fermentation of corn. These vegetable-derived forms are chemically identical to shellfish-derived glucosamine and are a safe alternative for individuals with severe shellfish allergies or those following strict vegan diets.¶ Mechanism of Action
Current research proposes several biological mechanisms explaining both the chondroprotective and systemic longevity effects of glucosamine.
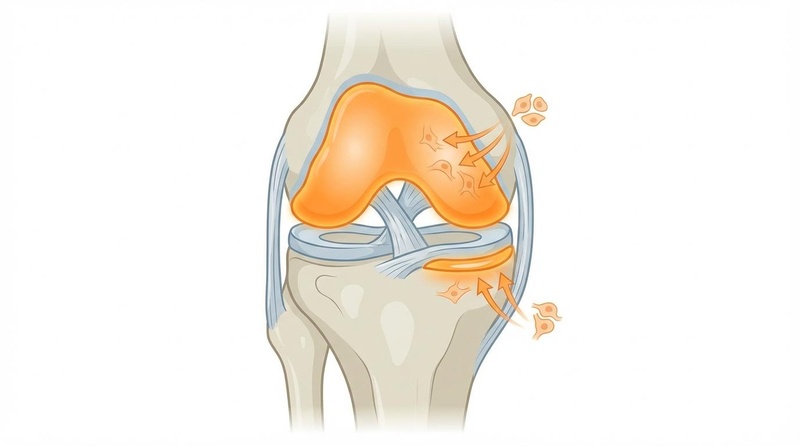
¶ Anti-Inflammatory Pathways (NF-κB Inhibition)
Glucosamine exhibits strong anti-inflammatory properties by inhibiting the Nuclear Factor-kappa B (NF-κB) signaling pathway. It prevents the intracellular cascade of Interleukin-1 beta (IL-1β), thereby reducing the production of pro-inflammatory cytokines (like IL-6 and TNF-α) and matrix metalloproteinases (MMPs) that are directly responsible for degrading cartilage [14][15]. This systemic reduction in chronic inflammation (e.g., lower C-reactive protein levels) is the leading hypothesis for the observed reductions in cardiovascular mortality [16].
¶ Autophagy and Longevity (mTOR/SIRT1)
Glucosamine appears to act as a calorie restriction mimetic, activating cellular pathways associated with lifespan extension:
- Autophagy Induction: Glucosamine induces autophagy (the cellular "cleanup" process) via the inhibition of the mTOR (mammalian target of rapamycin) pathway. This mechanism has been demonstrated to extend lifespan in C. elegans and aging mouse models [17][18].
- SIRT1 Activation: Glucosamine upregulates SIRT1 (Sirtuin 1), a critical longevity gene. SIRT1 deacetylates and inactivates p53, promoting cell survival, mitochondrial biogenesis, and metabolic flexibility [19].
¶ Evidence Summary Table (Human Outcomes)
| Outcome of Interest | Study Type | Key Findings | Certainty of Evidence (GRADE) | Citations |
|---|---|---|---|---|
| Knee OA: Pain Reduction (Sulfate form) | Meta-Analysis (RCTs) | Crystalline glucosamine sulfate is superior to placebo for pain (SMD -1.11) and function. | High | [6:1][2:1] |
| Knee OA: Pain Reduction (Hydrochloride form) | Meta-Analysis (RCTs) | Glucosamine HCl shows no clinically significant benefit over placebo for pain. | Moderate | [9:1][10:1] |
| Knee OA: Structural Modification | Meta-Analysis (RCTs) | Prescription CGS may delay joint space narrowing over 3 years; results inconsistent across non-prescription formulations. | Low | [3:1][6:2] |
| Cardiovascular Mortality Reduction | Prospective Cohort | Regular use associated with a 15% lower risk of CVD events and a 22% reduction in CVD mortality (UK Biobank). | Low | [4:1][20] |
| All-Cause Mortality Reduction | Prospective Cohort | Regular use (1+ years) associated with a ~39% reduction in all-cause mortality (NHANES data). | Low | [5:1][21] |
| Safety: Warfarin Interaction | Pharmacovigilance | Significant association with elevated INR and bleeding risk when co-administered with warfarin. | Moderate | [22][23] |
| Safety: Adverse Events (General) | Meta-Analysis (RCTs) | No significant difference in adverse events compared to placebo; generally well-tolerated. | High | [6:3][24] |
¶ Comprehensive Safety & Toxicology
Glucosamine has an excellent overall safety profile with a very low risk of toxicity, comparable to placebo in most clinical trials [6:4].
¶ Adverse Effects
When side effects occur, they are typically mild and gastrointestinal in nature. They may include:
- Nausea or dyspepsia (indigestion)
- Heartburn
- Diarrhea or constipation
- Mild abdominal pain [13:1]
¶ Critical Drug Interactions
- Warfarin (Coumadin): This is a heavily documented and potentially dangerous interaction. Multiple pharmacovigilance reports confirm that glucosamine can significantly potentiate the anticoagulant effect of warfarin. Case reports show INR (International Normalized Ratio) increases from a stable 2.5 to dangerously high levels (>4.0 or even >10.0) occurring 1–4 weeks after initiating glucosamine. INR typically returns to baseline upon discontinuation. The exact mechanism is unknown, but patients on warfarin should strictly avoid glucosamine or undergo frequent INR monitoring [22:1][23:1][25].
¶ Metabolic Considerations
Early animal models injected with massive doses of glucosamine showed signs of insulin resistance. However, robust human clinical trials have consistently demonstrated that oral glucosamine supplementation (1,500 mg/day) has no clinically significant effect on fasting blood glucose, insulin sensitivity, or HbA1c levels in healthy individuals or those with controlled type 2 diabetes [26]. Diabetic patients should still practice standard glucose monitoring when introducing new supplements.
¶ Compare With
- Chondroitin Sulfate: Often paired with glucosamine. Chondroitin is a larger molecule that helps cartilage retain water. While the combination is popular, network meta-analyses suggest glucosamine alone (as crystalline sulfate) or combined with Omega-3s may be more effective for pain, though chondroitin may offer complementary structural support [27].
- MSM (Methylsulfonylmethane): An organic sulfur compound used for joint pain. MSM primarily acts as an anti-inflammatory and antioxidant. It is often combined with glucosamine, but the standalone clinical evidence for MSM in osteoarthritis is less robust than for glucosamine sulfate.
- Omega-3 Fatty Acids (EPA/DHA): Omega-3s address joint pain purely through systemic reduction of inflammatory cytokines (like PGE2). Glucosamine provides structural building blocks alongside localized anti-inflammatory signaling. Recent data suggests their combination is highly synergistic for joint health [27:1].
¶ References
Vangsness, C. T., et al. (2009). Review of Glucosamine and Chondroitin in the Management of Osteoarthritis. https://pmc.ncbi.nlm.nih.gov/articles/PMC5241539/ ↩︎
Towheed, T. E., et al. (2000). Glucosamine therapy for treating osteoarthritis: Cochrane Review. https://www.researchgate.net/publication/12053296_Glucosamine_therapy_for_treating_osteoarthritis_Cochrane_Review ↩︎ ↩︎
Reginster, J. Y., et al. (2001). Meta-analysis of glucosamine sulfate and glucosamine hydrochloride structure-modifying trials. https://www.researchgate.net/figure/Meta-analysis-of-glucosamine-sulfate-and-glucosamine-hydrochloride-structure-modifying_fig3_230592254 ↩︎ ↩︎
Ma, H., et al. (2019). Association of habitual glucosamine use with risk of cardiovascular disease: prospective study in UK Biobank. https://www.bmj.com/content/365/bmj.l1628 ↩︎ ↩︎
King, D. E., & Xiang, J. (2020). Glucosamine/Chondroitin and Mortality in a US NHANES Cohort. https://pmc.ncbi.nlm.nih.gov/articles/PMC8366581/ ↩︎ ↩︎
Towheed, T. E., et al. (2005). Glucosamine therapy for treating osteoarthritis. Cochrane Database of Systematic Reviews. https://www.cochrane.org/evidence/CD002946_glucosamine-osteoarthritis ↩︎ ↩︎ ↩︎ ↩︎ ↩︎
Saengnipanthkul, S., et al. (2019). Differentiation of patented crystalline glucosamine sulfate. International Journal of Rheumatic Diseases. https://www.esceo.org/sites/esceo/files/pdf/Differentiation of patented crystalline glucosamineSaengnipanthkul_et_al-2019-International_Journal_of_Rheumatic_Diseases.pdf ↩︎
Arden, N. K., et al. (2021). Non-surgical management of knee osteoarthritis: comparison of ESCEO and OARSI 2019 guidelines. https://www.esceo.org/sites/esceo/files/pdf/OA ESCEO OARSI GUIDELINES NRR 2021.pdf ↩︎
Eriksen, P., et al. (2014). Structural and symptomatic efficacy of glucosamine and chondroitin in knee osteoarthritis: a comprehensive meta-analysis. https://pmc.ncbi.nlm.nih.gov/articles/PMC3392795/ ↩︎ ↩︎
Cochrane Library. (2013). Glucosamine therapy for treating osteoarthritis. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK73794/ ↩︎ ↩︎
Kolasinski, S. L., et al. (2020). 2019 American College of Rheumatology/Arthritis Foundation Guideline. https://pmc.ncbi.nlm.nih.gov/articles/PMC10518852/ ↩︎
Oulu University. (2020). Non-surgical management of knee osteoarthritis: comparison of ESCEO and OARSI 2019 guidelines. https://oulurepo.oulu.fi/bitstream/10024/30805/1/nbnfi-fe2020102988778.pdf ↩︎
Bolt Pharmacy. (2026). Recommended Glucosamine Dosage Per Day for Adults. https://www.boltpharmacy.co.uk/guide/glucosamine-dosage-per-day ↩︎ ↩︎
Zhu, X., et al. (2019). Mechanisms of Glucosamine in the Management of Osteoarthritis. https://pdfs.semanticscholar.org/84da/0c8f047bd02d2d8998d8fa8362dcaf3f454d.pdf ↩︎
Reginster, J. Y. (2007). Glucosamine sulfate for knee osteoarthritis: Science and evidence-based use. https://www.openaccessjournals.com/articles/glucosamine-sulfate-for-knee-osteoarthritis-science-and-evidencebased-use.pdf ↩︎
Pyhtila, J. (2021). Glucosamine/Chondroitin Linked to Lower All-Cause and Cardiovascular Mortality. https://medium.com/lazarus-ai/glucosamine-chondroitin-linked-to-lower-all-cause-and-cardiovascular-mortality-1533bce5970b ↩︎
Carames, B., et al. (2013). Glucosamine activates autophagy in vitro and in vivo. https://pmc.ncbi.nlm.nih.gov/articles/PMC3772083/ ↩︎
Shintani, T., et al. (2018). Glucosamine Extends Lifespan of C. elegans via Autophagy. https://pmc.ncbi.nlm.nih.gov/articles/PMC8056925/ ↩︎
Shintani, T., et al. (2018). Molecular Mechanism for the Autophagy-Inducing Action of Glucosamine in Chondrocytes. https://pdfs.semanticscholar.org/6ed7/3275f6a92bebdb4e0058ff06e5175e7e9c78.pdf ↩︎
Ma, H., et al. (2019). Association of habitual glucosamine use with risk of cardiovascular disease: prospective study in UK Biobank. https://pubmed.ncbi.nlm.nih.gov/32253185/ ↩︎
King, D. E., & Xiang, J. (2020). Glucosamine/Chondroitin and Mortality in a US NHANES Cohort. https://pubmed.ncbi.nlm.nih.gov/33219063/ ↩︎
Health Sciences Authority. (2009). Reports of Warfarin-Glucosamine Interaction. https://www.hsa.gov.sg/announcements/safety-alert/reports-of-warfarin-glucosamine-interaction ↩︎ ↩︎
GPnotebook. (2019). Glucosamine and Warfarin Interaction. https://gpnotebook.com/en-GB/pages/rheumatology/glucosamine-and-warfarin ↩︎ ↩︎
Al-Hatamleh, M. A. I., et al. (2023). Efficacy and Safety of Glucosamine in Osteoarthritis: A Systematic Review. https://www.preprints.org/manuscript/202306.0475/v1 ↩︎
Drugs.com. (n.d.). Glucosamine with Warfarin Drug Interactions. https://www.drugs.com/drug-interactions/glucosamine-with-warfarin-1182-0-2311-0.html?professional=1 ↩︎
Tannis, A. J., et al. (2004). Effect of glucosamine supplementation on fasting and non-fasting plasma glucose. https://pmc.ncbi.nlm.nih.gov/articles/PMC3456914/ ↩︎
MDPI. (2024). Systematic Review and Network Meta-Analysis of Glucosamine. https://www.mdpi.com/2077-0383/13/23/7444 ↩︎ ↩︎
Comments
Discussion