Vitamin D3 and K2 are frequently co-supplemented due to their synergistic roles in calcium homeostasis. While Vitamin D promotes the absorption of calcium from the intestine, Vitamin K2 (specifically menaquinones like MK-4 and MK-7) directs that calcium into bone and keeps it out of soft tissues. This partnership is hypothesized to resolve the "Calcium Paradox"—the phenomenon where calcium supplements can simultaneously improve bone density while increasing the risk of arterial calcification.
¶ At a Glance
- The Synergy: Vitamin D3 "loads" the gun (increases calcium absorption and protein production), while Vitamin K2 "pulls the trigger" (activates proteins to direct calcium).
- Key Benefits: Improved bone mineral density (BMD) and reduced arterial stiffness.
- Longevity Link: Combined deficiency is associated with a 46% higher risk of all-cause mortality compared to adequate levels of both.
- Safety Warning: Vitamin K2 interferes with Warfarin/Coumadin. Patients on anticoagulants must consult a doctor.
¶ Mechanism of Action: The Calcium Synergy
The physiological basis for combining these vitamins lies in the activation of Vitamin K-dependent proteins (VKDPs).
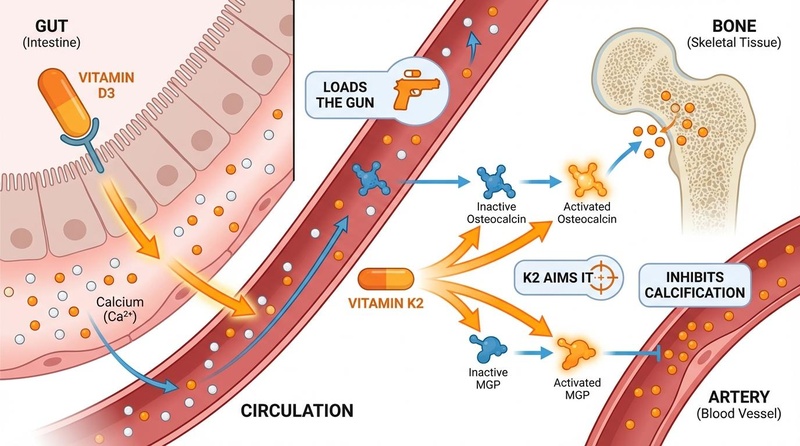
Figure 1: Vitamin D3 enhances calcium absorption, while Vitamin K2 activates Osteocalcin and MGP to direct calcium into bone and away from arteries.
¶ 1. Vitamin D3 (The Loader)
Vitamin D3 (cholecalciferol) converts to its active hormone form, calcitriol, which:
- Increases Absorption: Upregulates calcium transport proteins (e.g., TRPV6) in the gut, maximizing calcium uptake from food.
- Stimulates Protein Synthesis: Induces the expression of Osteocalcin (in bone) and Matrix Gla Protein (MGP) (in blood vessels). Crucially, D3 stimulates the production of these proteins, but they are released in an inactive, undercarboxylated form[1].
¶ 2. Vitamin K2 (The Director)
Vitamin K2 acts as an essential cofactor for the enzyme -glutamyl carboxylase. This enzyme activates the proteins created by Vitamin D3 via carboxylation (adding a carboxyl group), allowing them to bind calcium:
- Osteocalcin Carboxylated Osteocalcin (cOC): Binds calcium tightly, integrating it into the hydroxyapatite matrix of the bone, increasing density and strength[2].
- Matrix Gla Protein Carboxylated MGP (cMGP): Actively inhibits the precipitation of calcium in arterial walls, heart valves, and other soft tissues. MGP is the most potent known inhibitor of soft tissue calcification[3].
The Risk of Imbalance: Without adequate Vitamin K2, high doses of Vitamin D3 may lead to an accumulation of inactive proteins (ucOC and dp-ucMGP) and elevated serum calcium that cannot be effectively utilized by bone, potentially depositing in arteries instead (The "Calcium Paradox")[4].
¶ Clinical Evidence
¶ Bone Health
Certainty of Evidence: Moderate to High
The combination of Vitamin D3 and K2 appears superior to D3 alone for maintaining bone quality and preventing fractures.
- Bone Mineral Density (BMD): A 2020 meta-analysis of 8 RCTs (971 subjects) found that combined supplementation significantly increased total BMD compared to Vitamin D alone. The combination also significantly decreased levels of undercarboxylated (inactive) osteocalcin[2:1].
- Fracture Risk: High-quality evidence supports the role of Vitamin K2 in reducing vertebral fracture rates. Japanese protocols utilizing high-dose MK-4 (45 mg/day) have historically shown strong fracture prevention, although lower dose MK-7 trials focus more on BMD maintenance[1:1][5].
¶ Cardiovascular Health
Certainty of Evidence: Moderate
The cardiovascular benefits center on preventing vascular calcification, a major predictor of cardiovascular mortality and biological aging.
- Prevention vs. Reversal: The AVADEC trial (2022), a landmark double-blind RCT, investigated D3+K2 in patients with aortic valve calcification. While it did not reverse established calcification in the general group, a significant benefit was observed in a subgroup with high baseline Coronary Artery Calcification (CAC score > 400). In these high-risk patients, the combination significantly slowed the progression of calcification compared to placebo[6][7].
- Arterial Stiffness: Low levels of both vitamins are associated with increased arterial stiffness and hypertension. A 2023 RCT in diabetic hemodialysis patients found that 375 g of Vitamin K2 significantly reduced the progression of arterial stiffness[3:1].
¶ Longevity and Mortality
Combined deficiency amplifies mortality risk, potentially accelerating aging processes.
- Mortality Risk: The PREVEND study (prospective cohort, n=4,742) found that subjects with low levels of both Vitamin D and Vitamin K had a 46% higher risk of all-cause mortality compared to those with adequate levels. This risk was significantly higher than the deficiency of either vitamin alone, suggesting a true synergistic impact on longevity[8].
- Biomarkers of Aging: Inactive MGP (dp-ucMGP) is considered a biomarker of vascular vitamin K status and an independent predictor of mortality. Supplementation effectively lowers this biomarker, theoretically reversing a component of vascular aging[9].
¶ Dosage and Forms

Figure 2: Sources of Vitamin D3 and K2 include fatty fish, eggs, cheese, and natto.
¶ Vitamin K2 Forms: MK-7 vs. MK-4
Vitamin K2 exists in several forms, with MK-7 and MK-4 being the most relevant for supplementation.
| Feature | Menaquinone-7 (MK-7) | Menaquinone-4 (MK-4) |
|---|---|---|
| Source | Bacterial fermentation (Natto) | Animal fats, conversion from K1, synthetic |
| Half-Life | ~72 hours | 1–2 hours |
| Dosing Frequency | Once daily | Requires 3x daily dosing |
| Bioavailability | High (micronutrient doses effective) | Low (requires milligram doses) |
| Typical Dose | 90–180 mcg/day | 45 mg/day (therapeutic) |
Recommendation: MK-7 is generally preferred for preventive/maintenance supplementation due to its long half-life, which allows for stable serum levels with convenient once-daily dosing[10][11].
¶ Recommended Ratios
While there is no universally established medical ratio, functional medicine protocols often suggest:
- Standard Protocol: ~100 mcg of Vitamin K2 (MK-7) for every 5,000–10,000 IU of Vitamin D3[12].
- Independent Threshold: Some experts argue that K2 activation is threshold-based. Once sufficient K2 (e.g., 100–180 mcg) is present to maximally carboxylate MGP and Osteocalcin, increasing D3 intake does not necessarily require a proportional increase in K2, provided the baseline K2 requirement is met[13].
¶ Safety and Contraindications
¶ Warfarin Interaction
CRITICAL WARNING: Vitamin K2 is a direct antagonist to Vitamin K Antagonists (VKA) like Warfarin (Coumadin).
- Warfarin works by inhibiting the recycling of Vitamin K to prevent clotting. Supplementing with K2 bypasses this blockade and can completely reverse the anticoagulant effect, leading to a risk of stroke or thrombosis.
- MK-7 is extremely potent in this regard; doses as low as 10 mcg can destabilize INR levels. Patients on VKA anticoagulants must typically avoid K2 supplements unless under strict medical supervision[14][15].
¶ General Safety
- Toxicity: Vitamin K2 has no established Upper Limit (UL) and no known toxicity in healthy individuals, even at high doses (e.g., 45 mg/day used in Japanese osteoporosis treatment).
- Hypercalcemia: While K2 directs calcium to bones, it does not prevent Vitamin D toxicity (hypercalcemia) if D3 is taken in massive overdose. Regular monitoring of serum 25(OH)D and calcium is recommended for high-dose D3 regimens[16].
¶ References
van Ballegooijen, A. J., et al. (2017). The Synergistic Interplay between Vitamins D and K for Bone and Cardiovascular Health: A Narrative Review. Int J Endocrinol. https://pmc.ncbi.nlm.nih.gov/articles/PMC5613455/ ↩︎ ↩︎
Kuang, X., et al. (2020). The combination effect of vitamin K and vitamin D on human bone quality: a meta-analysis of RCTs. Food & Function. https://pubmed.ncbi.nlm.nih.gov/32219282/ ↩︎ ↩︎
Hariri, E., et al. (2021). Vitamin K2—a neglected player in cardiovascular health: a narrative review. Open Heart. https://openheart.bmj.com/content/8/2/e001715 ↩︎ ↩︎
Dr. Oracle. (2025). Is Vitamin D3 + K2 better than D3 alone for vascular calcification? https://www.droracle.ai/articles/251400/is-vitamin-d3-k2-vitamin-d3-vitamin ↩︎
SciELO. (2015). Vitamin K and Bone Health. https://scielo.isciii.es/pdf/romm/v7n1/en_revision2.pdf ↩︎
Diederichsen, A. C. P., et al. (2022). Vitamin K2 and D in Patients With Aortic Valve Calcification: A Randomized Double-Blinded Clinical Trial. Circulation. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.121.057008 ↩︎
Nutraceuticals World. (2024). Vitamin K2 and D may be beneficial in coronary artery calcification. https://www.nutraceuticalsworld.com/breaking-news/vitamin-k2-and-d-may-be-beneficial-in-coronary-artery-calcification/ ↩︎
van Ballegooijen, A. J., et al. (2020). Combined low vitamin D and K status amplifies mortality risk: a prospective study. Eur J Nutr. https://pubmed.ncbi.nlm.nih.gov/32808059/ ↩︎
Hasific, S., et al. (2023). Effects of vitamins K2 and D3 supplementation in patients with severe coronary artery calcification. BMJ Open. https://pmc.ncbi.nlm.nih.gov/articles/PMC10351276/ ↩︎
Sato, T., et al. (2012). Comparison of menaquinone-4 and menaquinone-7 bioavailability in healthy women. Nutr J. https://pmc.ncbi.nlm.nih.gov/articles/PMC3502319/ ↩︎
Mediq7. Which one is the best form for Vitamin K2? https://www.mediq7.com/blog/which-one-is-the-best-form-for-vitamin-k2/ ↩︎
Dr. Berg. (2023). Best ratio of vitamin D3 to K2 for optimal health. https://www.drberg.com/blog/best-ratio-of-vitamin-d3-to-k2-for-optimal-health ↩︎
Vitamin Express. (2022). How to combine Vitamin D and Vitamin K properly. https://www.vitaminexpress.org/en/how-to-combine-vitamin-d-and-vitamin-k-properly ↩︎
Theuwissen, E., et al. (2013). Low-dose menaquinone-7 supplementation significantly decreases INR in patients on acenocoumarol. Blood. https://pubmed.ncbi.nlm.nih.gov/23530987/ ↩︎
Drugs.com. Vitamin K2 with Warfarin Interaction. https://www.drugs.com/drug-interactions/vitamin-k2-with-warfarin-4087-19568-2311-0.html ↩︎
NCBI Bookshelf. Vitamin K. https://www.ncbi.nlm.nih.gov/books/NBK551578/ ↩︎
Comments
Discussion